Conception Calculator
Free Conception Calculator: find your exact ovulation date, 6-day fertile window, and peak conception days based on your last period and cycle length....
????? ???? ??? ?????
How to Use the Conception Calculator
Enter the first day of your last menstrual period (LMP), your average cycle length, and your estimated luteal phase length. Click Calculate Fertile Window to instantly see your predicted ovulation date, six-day fertile window, peak conception days, and next expected period. The calculator also generates a visual 12-month conception calendar so you can plan intercourse on your most fertile days.
For best accuracy: use the first day of your last period — the day bleeding actually started, not spotting. If your cycle length varies, use the average of your last 3–6 cycles. The default luteal phase of 14 days is accurate for most women; adjust if you track basal body temperature (BBT) and know your own luteal length. If you are unsure of your cycle length, 28 days is a reasonable starting estimate for most people.
Step-by-Step Instructions
- Enter your last period date — the first full bleeding day of your most recent menstrual period.
- Set your cycle length — the average number of days from the first day of one period to the first day of the next. Most women range from 21 to 35 days.
- Adjust luteal phase — the number of days between ovulation and the start of your next period. The luteal phase is relatively fixed at 12–16 days for most women. The default of 14 days is standard.
- Click Calculate Fertile Window — your ovulation date, fertile window, and best conception days are instantly displayed with a probability chart.
- Plan intercourse — aim for 2–3 days before ovulation through ovulation day for maximum conception probability.
The Science of Ovulation and Conception Timing
Conception requires the meeting of a viable egg and viable sperm in the fallopian tube within a precisely timed window. Understanding the biology behind this window is essential for maximizing your chances — and for appreciating why timing matters so much in natural conception.
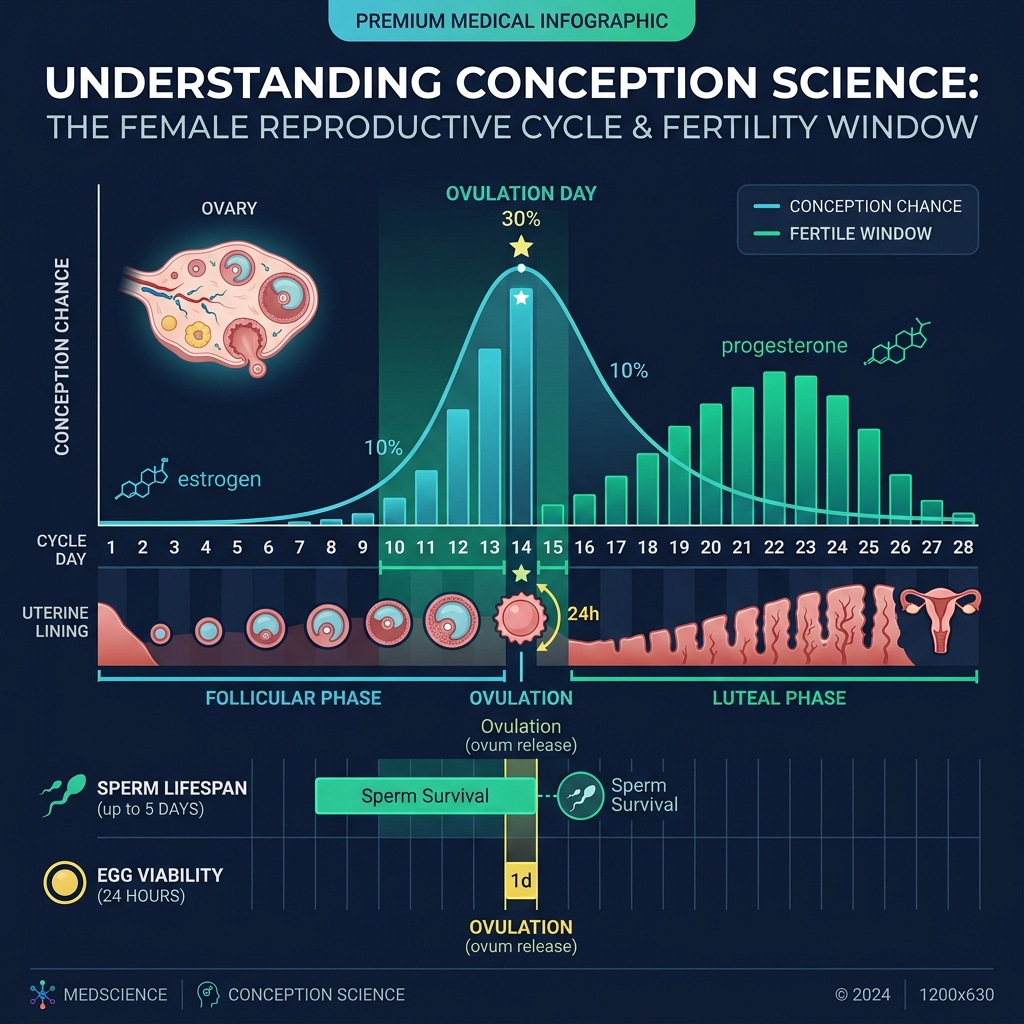
The Menstrual Cycle and Ovulation
The menstrual cycle is divided into two phases by the event of ovulation:
- Follicular Phase (Day 1 to Ovulation): The hypothalamus releases GnRH (gonadotropin-releasing hormone), which triggers the pituitary gland to release FSH (follicle-stimulating hormone). FSH stimulates the ovaries to develop follicles, with one becoming the dominant follicle. Rising estrogen levels from the growing follicle eventually trigger an LH (luteinizing hormone) surge, which causes ovulation — the release of a mature egg — typically 24–36 hours after the LH surge begins. The follicular phase is the variable part of the cycle; it is longer in women with longer cycles.
- Luteal Phase (Ovulation to Next Period): After the egg is released, the ruptured follicle transforms into the corpus luteum, which produces progesterone to prepare the uterine lining for implantation. If fertilization does not occur, the corpus luteum degenerates after 12–16 days, progesterone drops, and menstruation begins. The luteal phase is relatively constant at 12–16 days — this predictability is what allows your cycle length to predict your ovulation date.
Egg Viability: The 12–24 Hour Window
Once released, a mature egg is viable for only 12–24 hours. This is the actual biological window during which fertilization must occur for pregnancy to result. However, this narrow window is compensated by sperm's extended lifespan inside the female reproductive tract.
Sperm Lifespan: The 5-Day Advantage
Healthy sperm can survive in the female reproductive tract for 3–5 days, and in some cases up to 6 days under favorable conditions (abundant fertile-quality cervical mucus). This creates the 6-day fertile window: the five days before ovulation when sperm deposited via intercourse can survive until the egg is released, plus ovulation day itself when fertilization is most likely.
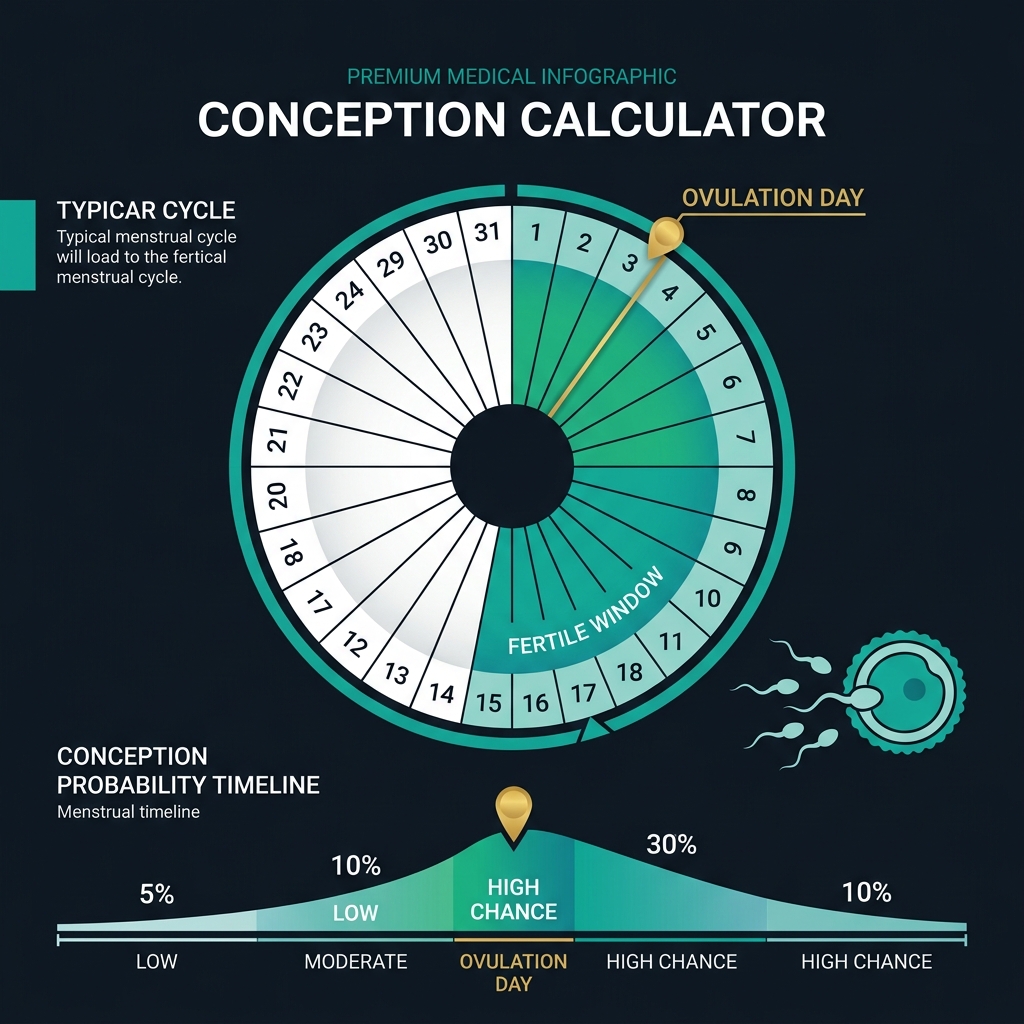
The Six-Day Fertile Window: Daily Conception Probabilities
Research published in the New England Journal of Medicine (Wilcox et al., 1995) and replicated in multiple subsequent studies provides the following daily conception probability estimates for a single act of unprotected intercourse:
- 5 days before ovulation: approximately 10% chance of pregnancy
- 4 days before ovulation: approximately 16% chance
- 3 days before ovulation: approximately 14%
- 2 days before ovulation: approximately 27%
- 1 day before ovulation: approximately 31% — the single most fertile day
- Ovulation day: approximately 33% (highest per-act probability due to concurrent egg viability)
- 1 day after ovulation: approximately 0–5% (egg viability typically exhausted)
These figures are per-act probabilities. Regular intercourse every 1–2 days during the full fertile window produces cumulative conception chances of 38–60% per cycle for a fertile couple under age 35, rising with each additional cycle.
How to Maximize Your Chances of Conception
Beyond timing intercourse with the fertile window, several evidence-based strategies can meaningfully improve your probability of conception each cycle.
Timing Strategy: The "Every Other Day" Rule
For most couples, the optimal strategy is intercourse every 1–2 days throughout the fertile window (5 days before through ovulation day). Daily intercourse during this window is also effective but not significantly superior, and may add psychological pressure. One large study found no statistically significant difference in conception rates between daily and every-other-day intercourse during the fertile window. The key insight: frequent intercourse beats perfect timing. Do not try to restrict intercourse to a single "optimal day" — sperm quality is better with slightly less frequency, but daily to every-other-day during the window maximizes cumulative probability.
Fertility Tracking Methods to Identify Your Actual Ovulation Date
Calendar-based prediction from cycle length is a starting point. For the most accurate real-time ovulation detection, consider these methods:
- LH Ovulation Test Strips: Over-the-counter LH surge test kits detect the LH spike that triggers ovulation 24–36 hours before it occurs. A positive LH test means ovulation is imminent — begin or continue daily intercourse immediately. Test in the afternoon (2–8 PM), when LH concentration is highest. A positive followed by a second test can confirm the LH surge has peaked.
- Basal Body Temperature (BBT) Charting: Progesterone released after ovulation raises resting body temperature by 0.2–0.5°C (0.4–1.0°F). Track your BBT daily before rising from bed — a sustained rise indicates ovulation has occurred. BBT charting confirms ovulation retrospectively and helps you understand your own luteal phase length for more precise future cycle predictions.
- Cervical Mucus Monitoring: Estrogen rising before ovulation changes cervical mucus texture from dry/sticky (non-fertile) to wet, clear, and stretchy — commonly described as resembling raw egg whites. This fertile-quality mucus is essential for sperm transport and survival. Peak mucus (the last day of egg-white discharge) corresponds closely with the most fertile days. Cervical mucus monitoring adds a biological real-time signal to calendar-based predictions.
- Symptothermal Method (BBT + Cervical Mucus): Combining BBT charting with cervical mucus monitoring — the symptothermal method — is the most accurate natural form of fertility tracking, with method failure rates of under 2% per year when correctly taught and applied. Certified fertility awareness educators can teach this method in clinical detail.
Male Factor Optimization
Approximately 40–50% of infertility cases involve a male factor component. Sperm quality can be improved through:
- Avoid heat: Testicular temperature is critical. Laptops on the lap, long hot baths, tight underwear, and heated car seats can impair sperm production for up to 3 months (the time it takes to complete a full sperm production cycle). Switch to loose-fitting cotton underwear and limit prolonged heat exposure.
- Alcohol and smoking: Both are associated with reduced sperm count, motility, and morphology. Reducing or eliminating alcohol and ceasing smoking improves semen parameters within 3 months. Estimates suggest smoking reduces male fertility by up to 15%.
- Supplements: Antioxidants including vitamin C (1,000 mg/day), vitamin E (400 IU/day), coenzyme Q10 (200–400 mg/day), zinc (25–50 mg/day), and selenium (100 mcg/day) have RCT evidence supporting improvements in sperm motility and DNA integrity in subfertile men. Folate is also important for reducing sperm DNA fragmentation.
- Abstinence interval: Sperm quality peaks after 2–5 days of abstinence. Less than 1 day or more than 7 days of abstinence is associated with reduced count or motility. For intercourse during the fertile window, 2–3 days between ejaculations optimizes the quality-to-quantity balance.
Female Factor Optimization
- Folic acid: Begin taking 400–800 mcg of folic acid (or a prenatal vitamin containing folate) at least 1 month before attempting conception. Folic acid dramatically reduces the risk of neural tube defects (NTDs) such as spina bifida — defects that form in the first 28 days after conception, often before pregnancy is even confirmed. This is the single most evidence-backed preconception supplement.
- BMI and weight: Both underweight (BMI <18.5) and overweight (BMI >30) significantly impair ovulation and conception probability. A BMI between 18.5 and 25 is consistently associated with optimal fertility. Even modest weight changes (5–10% of body weight) can restore ovulation in anovulatory women with PCOS or hypothalamic amenorrhea. Use our BMI Calculator to check your current status.
- Exercise: Excessive high-intensity exercise (especially combined with low caloric intake) can suppress the HPG axis and cause hypothalamic amenorrhea — particularly in endurance athletes. Moderate exercise (150 minutes of moderate activity per week) supports fertility. Reduce intensity if cycle disruption is suspected.
- Alcohol: Even moderate alcohol consumption has been associated with reduced fecundability in several prospective studies. Current guidelines for women trying to conceive recommend avoiding alcohol entirely.
- Sleep and stress: Sleep deprivation and chronic stress can disrupt GnRH pulsatility, delaying ovulation. Prioritize 7–9 hours of sleep and use structured stress management (mindfulness, yoga, cognitive behavioral therapy) during the conception journey.
How Age Affects Conception
Age is the most significant biological factor affecting natural conception probability. Female fertility peaks in the early-to-mid 20s and declines gradually through the late 20s, then more steeply after 32, and dramatically after 37. The primary driver is oocyte (egg) quantity and quality. Women are born with approximately 1–2 million eggs; by puberty this is reduced to 300,000–400,000; and by the mid-30s, the remaining eggs decline in quality (increased chromosomal abnormalities) and quantity.
- Under 25: Monthly fecundability approximately 25–30%, with approximately 90% of couples conceiving within 12 months of trying.
- 25–29: Monthly fecundability approximately 20–25%; 86% conceive within 12 months.
- 30–34: Monthly fecundability approximately 15–20%; 78% conceive within 12 months.
- 35–39: Monthly fecundability approximately 10–15%; 63% conceive within 12 months. ACOG recommends evaluation after 6 months of trying at this age.
- 40–44: Monthly fecundability approximately 5–10%; 36% conceive spontaneously within 12 months. Medical consultation is warranted from the start.
Male fertility also declines with age — gradually from age 40, more significantly after 45 — but is less dramatic than female age-related changes.
When to See a Doctor
Conception timing tools are an excellent starting point but are not a substitute for professional evaluation when clinical indicators are present. Consult a reproductive medicine specialist (REI) or ob-gyn in these circumstances:
- Under 35: after 12 months of regular, unprotected intercourse without pregnancy
- 35–37: after 6 months of trying
- Over 38: immediately upon deciding to conceive
- Any person with irregular or absent periods (possible PCOS, hypothalamic amenorrhea, or other ovulatory dysfunction)
- Known history of endometriosis, pelvic inflammatory disease, uterine fibroids, or prior ectopic pregnancy
- Male partner with known varicocele, prior sexually transmitted infections, or chemotherapy/radiation exposure
- More than 2 prior miscarriages (recurrent pregnancy loss warrants investigation after 2 losses, not 3)
A basic fertility workup typically includes cycle day 3 FSH, LH, and AMH bloodwork; antral follicle count ultrasound; and a semen analysis. These tests are inexpensive relative to assisted reproduction cycles and provide critical information for treatment planning. Use our Age Calculator to confirm your exact age for clinical reference purposes.
Related Health Calculators
Conception is one step in your complete reproductive health journey. Use these related tools for comprehensive planning:
- Period Calculator — Predict your next 6 menstrual periods, track cycle phases, and identify fertile windows over multiple months
- BMI Calculator — Optimal BMI (18.5–24.9) is directly associated with higher ovulation frequency and conception probability
- Age Calculator — Know your exact age for appropriate fertility evaluation timelines and risk stratification
- Ideal Weight Calculator — Reaching healthy weight is among the most effective lifestyle interventions for restoring ovulation
- Maintenance Calorie Calculator — Adequate caloric intake prevents hypothalamic amenorrhea, which affects fertility in under-eating women and athletes
- Harris-Benedict Calculator — Calculate your basal metabolic rate to ensure you are consuming enough calories to support healthy hormone function
- Blood Sugar Converter — Insulin resistance and diabetes affect ovulation; monitoring blood glucose is relevant for women with PCOS